 Home >
Solutions - Microwave Ablation - MWA in Kidney
Home >
Solutions - Microwave Ablation - MWA in Kidney
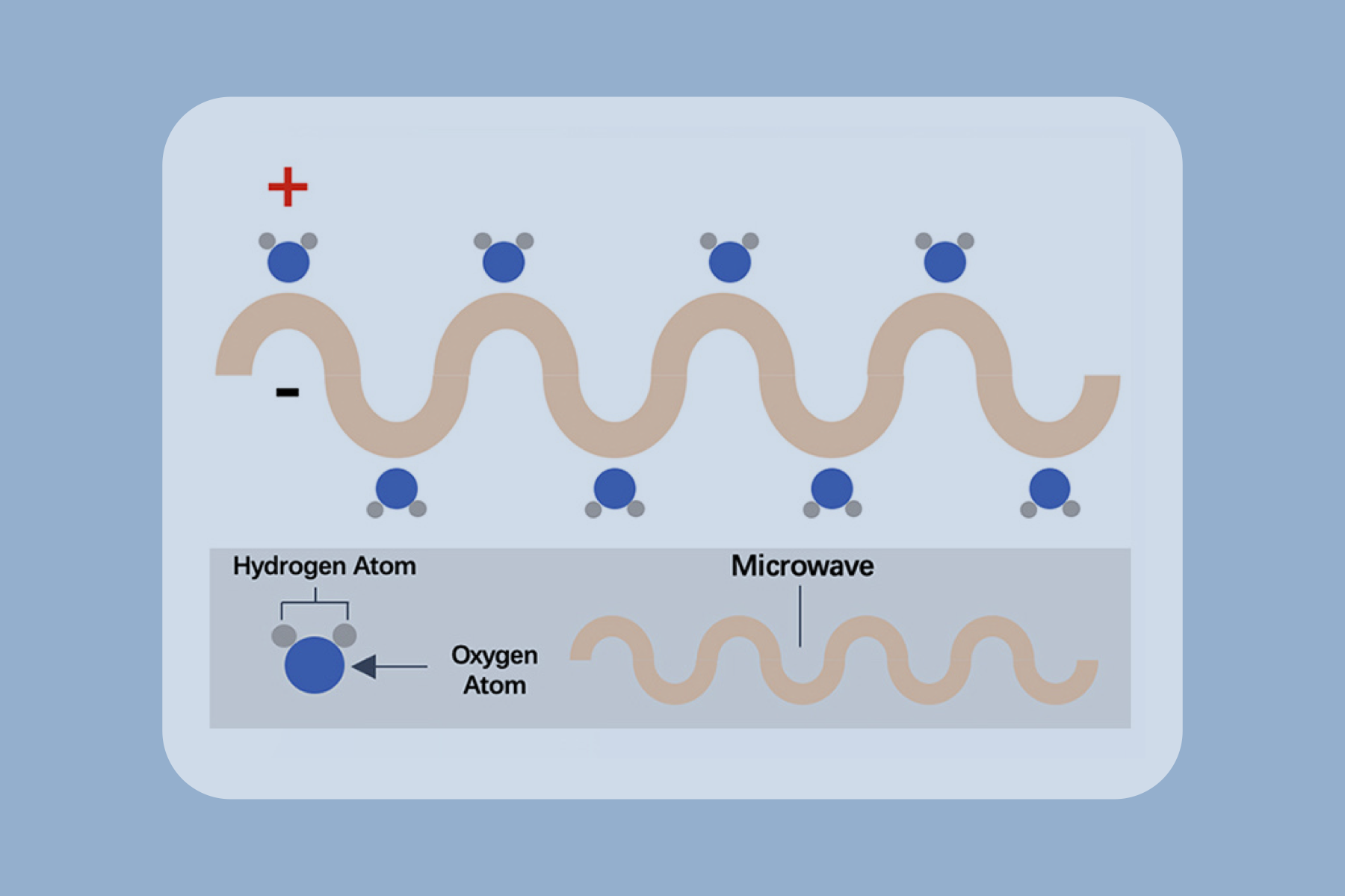
Microwave ablation refers to the use of the electromagnetic methods for inducing tumor destruction by using devices with frequencies of at least 900 MHz to produce tissue-heating effects [6]. Currently, 2450MHz is the frequency used by mainstream products worldwide.

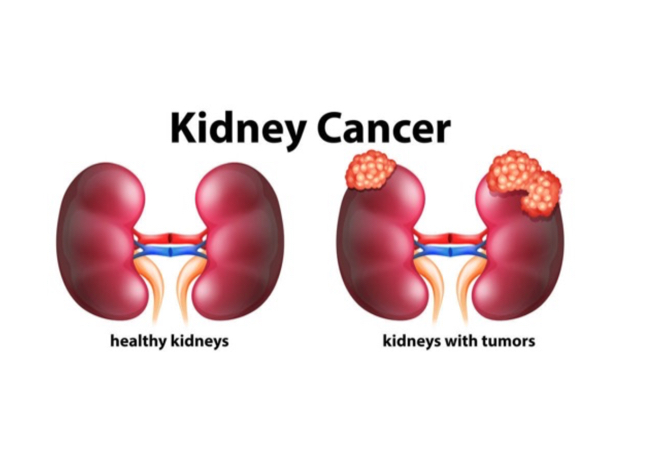
MWA in a 45-year-old man with right RCC adjacent to the renal pelvis. (a) Preablation arterial phase magnetic resonance imaging (MRI) scan shows one heterogeneous enhancement of neoplasm (arrow) near the renal pelvis with the size of 2.4 × 19. cm. (b) Arterial phase MRI scan obtained 2 months after ablation shows hypoattenuating ablation zone (arrow) without enhancement. (c) Scan obtained 12 months after ablation shows hypoattenuating ablation zone (arrow) without enhancement corresponding to treated region. (d) Scan obtained 24 months after ablation shows diminishing hypoattenuating ablation zone (arrow) without enhancement [10].
Advantages
Reduced morbidity and mortality

Suitability for real-time imaging guidance

Less invasive & short hospitalization stay

Synergy with other cancer treatments
Repeatability
Cost effectively









 Video
Video