'Save your thyroid'
 Home >
Solutions - Microwave Ablation - MWA in Thyroid
Home >
Solutions - Microwave Ablation - MWA in Thyroid
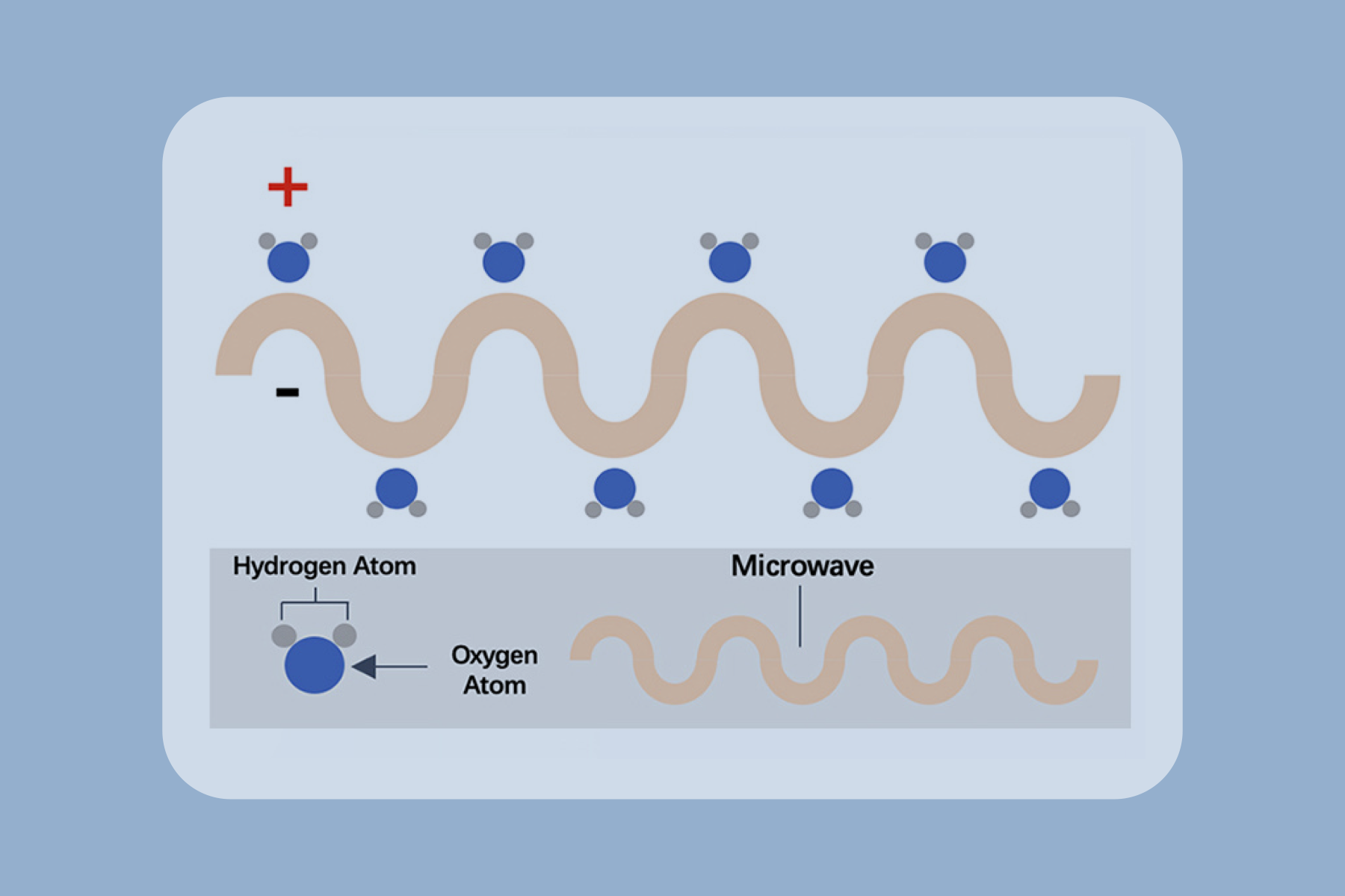
Microwave ablation refers to the use of the electromagnetic methods for inducing tumor destruction by using devices with frequencies of at least 900 MHz to produce tissue-heating effects [4]. Currently, 2450MHz is the frequency used by mainstream products worldwide.

US images in a 36-year-old man with papillary thyroid carcinoma in the right lobe of the thyroid [9]. (A) Preablation image of the tumor (arrowheads). (B) The hydrodissection technique (arrows) was used to protect the carotid artery (a) and vagus nerve. (C) Hyperechoic pattern in the tumor during the ablation procedure(arrowheads). (D) Postablation contrast-enhanced image shows no enhancement in the tumor area (arrowheads). (E) Image of the ablation zone 6 months after ablation (arrowheads). (F) The ablation area has almost disappeared 1 year after ablation.
Advantages
High cosmetic score and less scarring

Shorter hospitalization stay

Little to no damage to healthy thyroid tissue, preserving the thyroid functions
Quicker recovery time

High success rate with low risk of complication
General anesthesia is not required








 Video
Video